SUMMARY OF JOURNAL ARTICLES ON PERIODONTITIS
DH 23 – Mrs. Callaghan
DESCRIPTION:
Periodontitis is defined as an inflammatory disease of the supporting tissues of the teeth caused by specific microorganisms or groups of specific microorganisms. It results in the progressive destruction of the periodontal ligament and the alveolar bone with periodontal pocket formation, gingival recession or both. It’s a disease of the periodontium that is characterized by the irreversible loss of connective attachment and supporting alveolar bone. The loss of connective tissue and bone support is a major cause of tooth loss in adults.
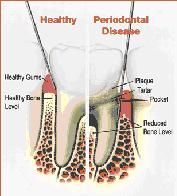
The structure of a healthy tooth and how it is typically affected by periodontal disease (picture source: American Academy of Periodontology; http://www.perio.org).
The structure of a healthy tooth and how it is typically affected by periodontal disease (picture source: American Academy of Periodontology; http://www.perio.org).
DISTINGUISHING DIAGNOSTIC FACTORS:
* In periodontitis, there is inflammation around the tooth and the gums pull away from the teeth and form spaces (called “pockets”) that become infected. The body’s immune system fights the bacteria as the plaque spreads and grows below the gum line. Bacterial toxins and the body’s natural response to infection start to break down the bone and connective tissue that hold the teeth in place. If not treated, the bones, gums, and tissue that support the teeth are destroyed. The teeth may eventually become loose and have to be removed.
* Purplish, red, or pale pink tissue color; swollen or fibrotic margin; papillae that do not fill embrasure spaces; bleeding upon gentle probing; may be pus; probe depth >4mm because of apical migration of junctional epithilium; bone loss; attachment loss.
* Purplish, red, or pale pink tissue color; swollen or fibrotic margin; papillae that do not fill embrasure spaces; bleeding upon gentle probing; may be pus; probe depth >4mm because of apical migration of junctional epithilium; bone loss; attachment loss.
ETIOLOGY OF PERIODONTITIS

Local contributing factors: Faulty restorations, crowded teeth.
Systemic contributing factors: Diabetes, smoking, puberty, pregnancy, medications.
Genetic risk factors: some people are more prone to severe gum disease than others periodontal tissues and
disease destruction.
(a) Diagram depicting a tooth with healthy periodontal tissues (cementum, connective tissue, and alveolar bone) on the left side and damaged tissues due to periodontal disease on the right side of the tooth.
(b) Radiograph of molar teeth. Local destruction of supporting alveolar bone due to periodontal disease is shown by the right arrow, while optimal bone levels are shown by the left arrow.
Systemic contributing factors: Diabetes, smoking, puberty, pregnancy, medications.
Genetic risk factors: some people are more prone to severe gum disease than others periodontal tissues and
disease destruction.
(a) Diagram depicting a tooth with healthy periodontal tissues (cementum, connective tissue, and alveolar bone) on the left side and damaged tissues due to periodontal disease on the right side of the tooth.
(b) Radiograph of molar teeth. Local destruction of supporting alveolar bone due to periodontal disease is shown by the right arrow, while optimal bone levels are shown by the left arrow.
PATHOGENS ASSOCIATED WITH PERIODONTITIS The pathogens that are significantly associated with periodontitis patients are gram-negative anaerobic bacteria classify in Socransky’s color such as Porphyromonas gingivalis, Actinobacillus actinomycetemcomitans, Tannerella forsythia, Treponema denticola, Prevotella intermedia/nigrescens and Fusobacterium nucleatum.
CLASSIFICATION OF PERIODONTITIS (using AAP classification system)
Class I - Gingival diseases
A. Denta plague-induced gingival diseases
B. Non-plague-induced gingival lesions
Class II - Chronic periodontitis
Slight: 1-2 mm CAL with 3-4 mm probing depths
Moderate: 3-4 mm CAL with 5-7 mm probing depths
Severe: >5 mm CAL with 7mm probing depths or greater
A. Localized (<30% of sites are involved)
B. Generalized (>30% of sites are involved)
Class III – Aggressive periodontitis (same as class II) occurs prior to age 35
Class IV – Periodontitis as a Manifestation of Systemic Diseases
A. Associated w/ hematological disorders
B. Associated w/ genetic disorders
C. Not otherwise specificed
Class V – Necrotizing Periodontal Diseases
Class VI – Abscesses of Periodontium
Class VII – Periodontitis associated with Endodontic Lesions
Class VIII – Developmental or Acquired Deformities and Conditions
PREVALENCE OF PERIODONTITIS
1% in group of 14-17 years old
4% in group of 18-34 years old
70% in-group of 35-44 years old
90% in-group of 45-80 years old
FACTORS TO INCLUDE IN PATIENT EDUCATION
* Explain to the patient the importance of good daily home care and regularly visiting a dental office for professional care, control systemic diseases.
* Suggest changing certain behaviors, such as quitting smoking, as a way to improve treatment outcome.
* In some studies, researchers showed that people with gum diseases were more likely to develop heart disease or have difficulty controlling blood sugar,
and other health problems.
* However, the facts are that controlling gum diseases can save patients teeth.
TREATMENT RECOMMENDATIONS : The main goal is to control the infection. Any type of treatment requires the patient to keep up good daily care at home such as brushing their teeth twice a day with fluoride toothpaste, flossing regularly to remove plaque between teeth and using perio-aids and mouthwash.
MAINTENANCE RECOMMENDATIONS: Maintain good daily home care including interdental aids used and regularly visit a dental office for professional care, quit smoking, and control systemic diseases.
REFFERENCES : www.nidcr.nih.gov/OralHealth/topics/GumDiseases/Periodontal GumDisease.htm
http://www.perio.org
Stingu, C., et al. (2012). Microbial profile of patients with periodontitis compared with healthy subjects. Quintessence Int. 2012; 43:e23-e31.
Tobita, M., & Mizuno, H. (2010). Periodontal Disease and Periodontal Tissue Regeneration. Current Stem Cell Research & Therapy, 2010, 5, 168-174.
CLASSIFICATION OF PERIODONTITIS (using AAP classification system)
Class I - Gingival diseases
A. Denta plague-induced gingival diseases
B. Non-plague-induced gingival lesions
Class II - Chronic periodontitis
Slight: 1-2 mm CAL with 3-4 mm probing depths
Moderate: 3-4 mm CAL with 5-7 mm probing depths
Severe: >5 mm CAL with 7mm probing depths or greater
A. Localized (<30% of sites are involved)
B. Generalized (>30% of sites are involved)
Class III – Aggressive periodontitis (same as class II) occurs prior to age 35
Class IV – Periodontitis as a Manifestation of Systemic Diseases
A. Associated w/ hematological disorders
B. Associated w/ genetic disorders
C. Not otherwise specificed
Class V – Necrotizing Periodontal Diseases
Class VI – Abscesses of Periodontium
Class VII – Periodontitis associated with Endodontic Lesions
Class VIII – Developmental or Acquired Deformities and Conditions
PREVALENCE OF PERIODONTITIS
1% in group of 14-17 years old
4% in group of 18-34 years old
70% in-group of 35-44 years old
90% in-group of 45-80 years old
FACTORS TO INCLUDE IN PATIENT EDUCATION
* Explain to the patient the importance of good daily home care and regularly visiting a dental office for professional care, control systemic diseases.
* Suggest changing certain behaviors, such as quitting smoking, as a way to improve treatment outcome.
* In some studies, researchers showed that people with gum diseases were more likely to develop heart disease or have difficulty controlling blood sugar,
and other health problems.
* However, the facts are that controlling gum diseases can save patients teeth.
TREATMENT RECOMMENDATIONS : The main goal is to control the infection. Any type of treatment requires the patient to keep up good daily care at home such as brushing their teeth twice a day with fluoride toothpaste, flossing regularly to remove plaque between teeth and using perio-aids and mouthwash.
MAINTENANCE RECOMMENDATIONS: Maintain good daily home care including interdental aids used and regularly visit a dental office for professional care, quit smoking, and control systemic diseases.
REFFERENCES : www.nidcr.nih.gov/OralHealth/topics/GumDiseases/Periodontal GumDisease.htm
http://www.perio.org
Stingu, C., et al. (2012). Microbial profile of patients with periodontitis compared with healthy subjects. Quintessence Int. 2012; 43:e23-e31.
Tobita, M., & Mizuno, H. (2010). Periodontal Disease and Periodontal Tissue Regeneration. Current Stem Cell Research & Therapy, 2010, 5, 168-174.
